


Training Curriculum 2022
Effective for trainees who enter training on or after 1/7/2022 (Version 18/2/2022)
Download:
•Training Curriculum 2016 (Effective from 26 April 2016)
•Training Curriculum 2020 (Effective from 1 January 2020)
•Training Curriculum 2022 (Effective from 1 July 2022)
Download: Training Curriculum Flowchart
A. Curriculum overview
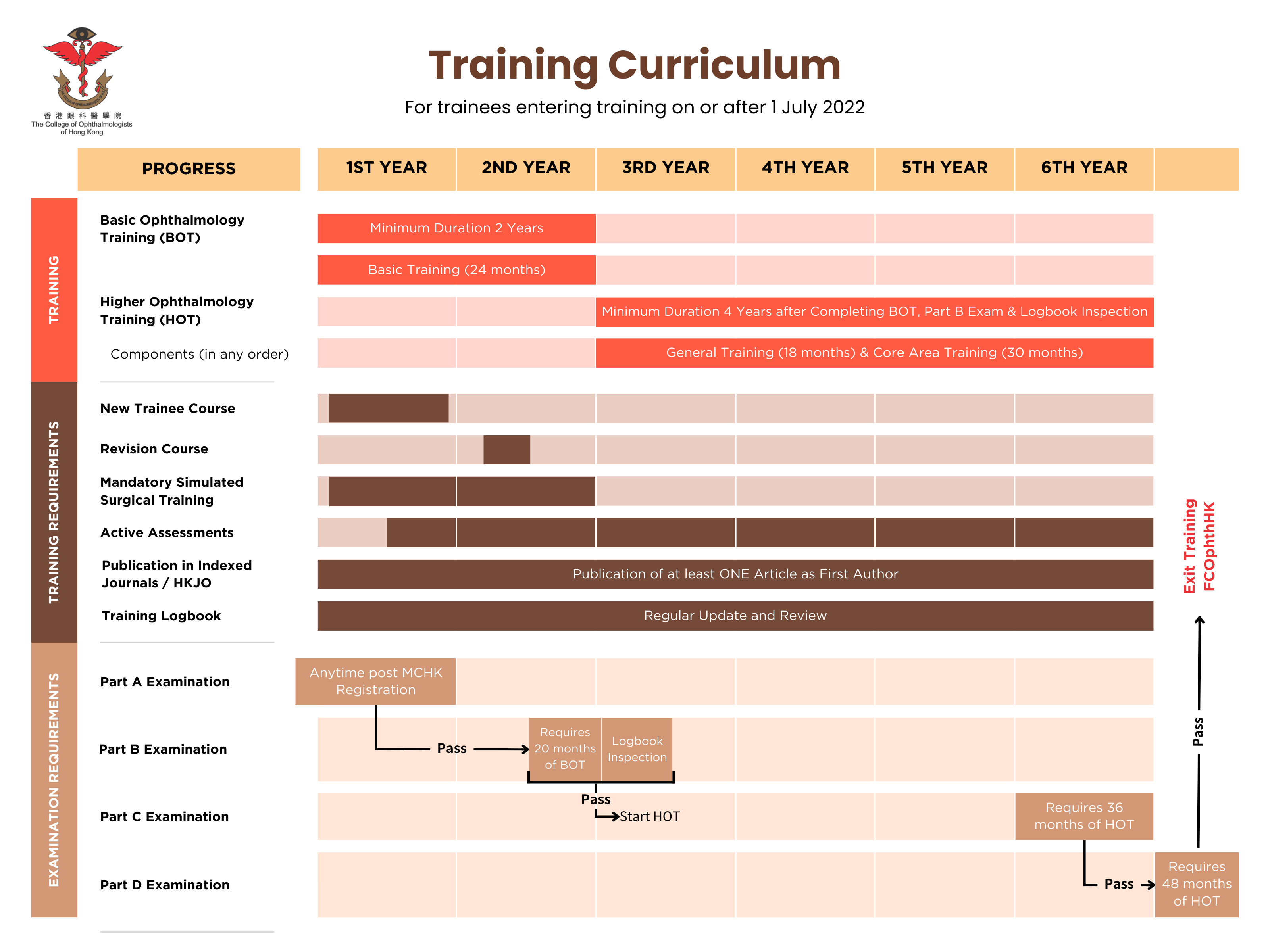
1. The training program has a minimum duration of 6 years, and the trainee must be in a College of
Ophthalmologists of Hong Kong (hereinafter referred to as “COHK”) recognized full-time training post in
ophthalmology in Hong Kong. For training centre requirements, please see the “Training Centre Accreditation
Guidelines”.
2. The training program is divided into two parts - Basic and Higher Training.
3. Basic Ophthalmology Training
a. The minimum duration is two years.
b. Basic Training is considered complete after the trainee has passed the intermediate examinations, has
undergone logbook inspection and satisfied the active assessment requirement.
4. Higher Ophthalmology Training
a. Higher Training can commence after completion of Basic Training.
b. The minimum duration is 4 years. It is further divided into general training (18 months minimum) and core area
training (minimum 6 months in each core area).
c. The core areas are:
ⅰ. Cornea and external eye diseases
ⅱ. Glaucoma
ⅲ. Oculoplastic and orbit
ⅳ. Paediatric ophthalmology and strabismus
ⅴ. Vitreo-retinal diseases
d. Higher Training is considered complete after the trainee has passed the exit examinations and satisfied the
active assessment requirement.
5. In addition, the following guidelines should be observed:
a. The period of training should preferably be continuous. Cumulative absence of less than 12 months throughout
the training period is acceptable. Additional training will be required for trainees whose accumulated leave
duration exceeds 12 months. All types of leave periods (including annual leave) are included. The trainee should
report the total number of leave days taken when he/she applies for the part C and part D examinations.
b. Any break of training for more than 12 cumulative months is not permitted, but the trainee may apply to the
College for exemption.
c. Research and overseas training in the field of ophthalmology is encouraged but whether the research or
overseas training can be considered as part of the training period will be left to the decision of COHK. However,
such periods should not be accredited for more than 12 months.
B. Training objectives
1. Basic Training
The aim of Basic Ophthalmology Training is for the general acquisition of ophthalmological knowledge, surgical
skills, and clinical judgement, as a continuous process, in stages under supervision that will enable the
ophthalmology trainee to handle general ophthalmic problems competently and at a high professional standard
at the end of Basic Training.
2. Higher Training
The aim of Higher Ophthalmology Training is for the acquisition of more advanced ophthalmic knowledge and
surgical skills in various subspecialties, such that at the end of Higher Training the trainee can handle more difficult
ophthalmic problems competently.
3. After completion of his/her training, the candidate is expected to be competent enough to become a general
ophthalmologist with or without a special interest in a subspecialty. Management and communication skills should
also be emphasized throughout the period of training.
C. Entry requirement
1. Basic Training (minimum 2 years)
a. The trainee applicant should be a registered medical practitioner with the Hong Kong Medical Council.
b. The trainee applicant should preferably have good-corrected eyesight, normal colour vision and good
binocularity to facilitate their training and their future career in ophthalmology.
2. Higher Training (minimum 4 years)
a. The candidate must meet all the requirements as for Basic Training.
b. The candidate should have completed his/her Basic Training successfully.
D. Examination structure
(Please refer to COHK website for prevailing examination guidelines for additional examination details)
1. Intermediate examination
a. Part A
• Format: written
• Prerequisite: The candidate must be registered with the Hong Kong Medical Council.
• If a candidate fails Part A four times, the candidate will not be allowed to sit for the examination again.
b. Part B
• Format: written, oral and clinical examination including practical refraction.
• Prerequisite: Passed Part A exam and completed of at least 20 months of Basic Ophthalmology Training.
• If a candidate fails half the stations or more, all stations of the Part B exam must be retaken. If a candidate fails
fewer than half of stations, only the concerned station(s) need(s) to be re-attempted.
• If a candidate fails Part B (one or more parts) four times, the candidate will not be allowed to sit for the
examination again.
2. Exit examination
a. Part C
• Format: 4 parts (written, critical appraisal of scientific publications, communication and clinical examinations)
• Prerequisite: Passed part B examination and completed of at least 3 years of Higher Training
• For Part C, if a candidate fails one part of the examination, only the concern part needs to be re-attempted.
However, if an overall pass cannot be achieved at the next sitting, or if the candidate fails more than one part,
all parts will need to be re-taken.
• If a candidate fails Part C (one or more parts) four times, the candidate will not be allowed to sit for the
examination again.
b. Part D
• Format: Logbook inspection and assessment
• Prerequisite: Passed part C examination and completed after at least 4 years of Higher Training
• If a candidate fails Part D four times, the candidate will not be allowed to sit for the examination again.
A trainee must complete his/her ophthalmology training (including all parts of the examination) within 12 years
unless he/she has been granted special permission by the COHK Education Committee.
E. Supervision, Trainer Definition & Responsibilities
(*Please refer to appendix for provisions for part-time trainers)
1. Definition of a trainer (general)
a. A trainer should have at least 2 years full-time (or full-time equivalent FTE)* working experience in COHK-
recognized training centers after obtaining:
ⅰ. Fellowship of COHK; or
ⅱ. The status of Specialist in Ophthalmology from the Medical Council of Hong Kong
b. Trainer: Trainee ratio
ⅰ. The overall trainer: trainee ratio is 1 trainer: 2 trainees maximum for a training centre.
ⅱ. For basic and general higher training, the trainer: trainee ratio is 1 trainer :2 trainees maximum.
ⅲ. One core area trainer (CAT, see below) can only supervise one higher ophthalmology trainee (HOT)
undergoing core area training at any one time. Therefore, one CAT can supervise one HOT (general training)
and one HOT (core area training), but not 2 HOTs (both core area training) simultaneously.
c. During the entire Higher Ophthalmology Training period, the trainee must be supervised by dedicated named
trainers.
d. An ophthalmologist employed full-time by the University of Hong Kong or the Chinese University of Hong Kong,
who has clinical duties at a training centre, are regarded as a full-time trainer in one training centre
e. Any trainer can be considered a full-time trainer or a named trainer in one training centre only.
2. Core area trainer (CAT) - see appendix for detailed definition of a core area trainer
a. During Higher Ophthalmology Training (4 years), the trainee must be supervised by a full-time or FTE named CAT
in all five core areas for at least 6 months each (total 2.5 years, see A4c for core areas). For the remaining 18
months of higher training, supervision by named trainers in any field of ophthalmology is permitted.
b. “Core area trainer” only applies to COHK training centers, it does not equate subspecialist status.
c. Rotation to other training centres to fulfil the training requirements is permitted.
d. One HOT cannot be trained in 2 core areas simultaneously.
3. Responsibilities of a trainer
a. Provide trainees with overall guidance in training and self-learning.
b. Monitor the progress of trainees to ensure that they meet the requirements of the training program.
c. Perform formative assessment and feedback to trainees periodically and at least every 6 months.
d. Provide support and career advice when appropriate.
F. Logbook
1. A trainee must keep a logbook or record of his/her operative experience and overall general performance. Regular
audits of surgical results are encouraged.
2. Logbooks should be obtained as soon as an ophthalmology trainee is accepted for training.
3. Accurate data entry is essential.
4. The logbook should be regularly reviewed by his/her trainers. At least yearly review of the logbook is required. COHK Education Committee reserves the right to conduct random checks on trainee logbooks.
G. Publication
1. The trainee is required to have at least one article (including original research, review articles, case reports and
meta-analyses; excluding letters to editor and photo essays) published in the Hong Kong Journal of
Ophthalmology or an indexed peer-reviewed journal.
2. The trainee needs to be the first (not co-first) author of the article.
3. Accurate data entry is essential.
4. The article (must be related to ophthalmology) concerned must be published (or accepted for publication) during
the training period and before the trainee attends the part D examination.
H. Acquisition of general knowledge and skills at various stages
Basic Training (minimum 2 years)
1. Diagnostics skills: acquisition and exposure to skills and knowledge in performing the following and accurate
interpretation of clinical signs observed by such:
a. Visual function tests:
ⅰ. Accurate assessment of patient’s visual acuity
ⅱ. Colour vision examination
ⅲ. Visual field examination
b. Refraction (Subjective and Objective)
c. Ophthalmic examination techniques, such as assessment of eye movement, eye lid position and function,
proptosis, pupils, directed general medical and neurological examination.
d. Biomicroscopic methods, such as slit-lamp, operating microscopy, tonometry, gonioscopy and slit lamp
fundoscopy and include the following:
ⅰ. Drawing of anterior segment findings
ⅱ. Interpret stains of the cornea and conjunctiva (e.g. Fluorescein and Rose Bengal)
ⅲ. Perform tests for dry eye (e.g. Schirmer test, tear film breakup)
ⅳ. Performance of Seidel test
e. Fundoscopy techniques such as direct and binocular indirect ophthalmoscopy with scleral indentation.
f. Detection, correlation and interpretation of relevant clinical findings and investigation of proper management of
patients. Discussion with patients and/or their relatives regarding their medical conditions and bedside etiquette
to enhance a patient-doctor relationship are emphasized.
g. Up-to-date knowledge of new investigative and operative instruments is strongly encouraged.
h. Exposure to other investigative or therapeutic procedures such as autorefraction, focimetry, keratometry, contact
lens fitting, low vision aids, orthoptic instrumentations, corneal topography, fundus photography, fluorescein and
indocyanine green angiography, ultrasonography, optical coherence tomography, electro-diagnostic
and neuroimaging techniques are expected.
i. Trainees are required to learn the basic principles of structural and microscopic changes of tissues in various
eye diseases and pathology, and the approach to therapy.
j. Understand different means of myopia control.
2. Surgical skills and operations:
a. The trainee is expected to have exposure to the following operations, mainly as an assistant, or occasionally
perform steps of the surgery under direct supervision of trainers:
ⅰ. Emergency operations
ⅱ. Intraocular operations including cataract extractions and glaucoma surgery
ⅲ. Extraocular operations, like lid mass, pterygium removal
ⅳ. Laser procedures (anterior segment, posterior segment, and glaucoma lasers)
b. At the end of this stage, the trainee is expected to have achieved the following clinical skills:
ⅰ. Competence in pre- and post-operative management of ophthalmic patients.
ⅱ. Acquisition of knowledge of giving premedication to ophthalmic patients and of obtaining preoperative
nformed consent by giving careful explanation to patients and/or their relatives of the possible outcome and
complications of individual operations.
ⅲ. Competence to perform minor procedures.
ⅳ. Acquisition of aseptic technique, proper draping, avoid external pressure on eyeball during operations etc.
ⅴ. Knowledge of ophthalmic surgical instruments and their respective usage. Careful handling of instruments is
strongly emphasized.
ⅵ. Acquisition of microsurgical techniques, instrumentation, and understanding of the maintenance and
operation of the microscope.
ⅶ. Performance of proper suturing techniques.
ⅷ. Attendance of eye emergencies.
ⅸ. Acquisition of various techniques of ophthalmic anaesthesia.
3. Exposure to various clinical areas, including:
a. Cornea and external eye diseases
b. Glaucoma
c. Neuro-ophthalmology
d. Oculoplastic and orbit
e. Ophthalmology related to general medicine
f. Paediatric ophthalmology and strabismus
g. Vitreoretinal diseases
4. Possession of proper professional ethics and conduct.
Higher Training (minimum 4 years)
Mainly a consolidation of the experience gained in both diagnostic skills and surgical skills during the Basic Training
period. Some supervision may be needed in the early stages. However, more and more surgical independence may
be granted as training progresses.
1. General skills
a. Perform cataract surgery, including extracapsular cataract extraction and phacoemulsification
b. Perform laser procedures (anterior segment, posterior segment, and glaucoma laser)
2. Clinical knowledge and skills:
Trainees are expected to rotate through various clinical areas to consolidate their training. These include:
a. Cornea and external eye diseases (including the principle and practice of refractive surgery)
b. Glaucoma
c. Oculoplastic and orbit
d.Ophthalmology related to general medicine
e. Neuro-ophthalmology
f. Paediatric ophthalmology and strabismus
g. Vitreoretinal diseases
During higher training, the trainee may choose a subspecialty of his/her special interest to prepare him/herself for
sub-specializing in a specific field. A period of overseas training and attendance of overseas conferences are
highly desirable during this stage. Research is also encouraged.
I. Simulated Surgical Training
1. Definition: Simulated surgical training is the use of simulated surgical environments for trainees to learn and
practice ophthalmic surgical procedures, or at least the key surgical steps of these procedures, prior to operating
on patients in an operating theatre setting.
2. Suitable material for suturing practice, artificial eye, animal eyes, cadaveric eyes or computer simulated
environment can all be used as media for simulated surgical training.
3. In general, all simulated surgical training must be conducted under the supervision of a COHK-approved trainer.
4. Mandatory simulated surgical training courses must follow the appropriate COHK guidelines for simulated surgical
training (if available) and must be approved by COHK, before it can be recognized as part of the trainee’s training.
5. During basic ophthalmology training, trainees are required to complete:
a. a basic surgical skills simulation course within 6 months after entering the COHK training program.
b. the following simulated laser courses before performing the respective procedures on patients:
c. At the end of this stage, the trainee is expected to have achieved the following clinical skills:
ⅰ. Anterior segment laser
ⅱ. Posterior segment laser
ⅲ. Glaucoma laser
d. simulated surgical training in other surgeries are not mandatory but highly recommended at different stages of
training, before performing the respective procedures on patients.
J. Practical skills requirement in different subspecialties
1. Cornea and External Eye Diseases
Topics to be covered in Basic Ophthalmology Training
a. Perform punctal occlusion (temporary or permanent) or insert plugs
b. Perform corneal sensation testing (e.g. cotton-tipped swab)
c. Perform techniques of sampling for viral, bacterial, fungal, and protozoal ocular infections (e.g. corneal scraping
and appropriate culture techniques)
d. Perform and interpret endothelial microscopy and pachymetry
e. Manage corneal epithelial defects (e.g. pressure patching and bandage contact lenses)
f. Perform removal of a conjunctival or corneal foreign body (e.g. rust ring, tarsal foreign body)
g. Perform pterygium surgery
h. Perform an isolated corneal laceration repair (e.g. linear laceration not extending to limbus, not involving uveal or
intraocular structures)
Topics to be covered in Higher Ophthalmology Training
a. Perform and interpret the most advanced corneal imaging and measurement techniques
b. Gunderson flap
c. Perform application of corneal glue
d. Perform stromal micropuncture
e. Assist lateral tarsorrhaphy
f. Assist more complex corneal surgery (e.g. penetrating or lamellar keratoplasty, keratorefractive procedures and
phototherapeutic keratectomy) and understand the postoperative management including post-keratoplasty
astigmatism management and graft rejection
g. Assist in collagen cross-linking
h. Management of intraoperative and postoperative complication of cataract extraction.
i. Perform secondary intraocular lens implantation
Refractive Surgery
Topics to be covered in Higher Ophthalmology Training
a. Able to perform preoperative assessment
ⅰ. Understand the indications and contraindications of refractive procedures
ⅱ. Keratoconus assessment / screening
ⅲ. Interpretation of corneal topography and wave front analysis
ⅲ. Assessment of phakic intraocular lens implantation
b. Understand the principles of the following refractive procedures:
ⅰ. Laser-Assisted in Situ Keratomileusis (LASIK)
ⅱ. Laser-Assisted in Situ Keratomileusis Extra (LASIK Extra)
ⅲ. Advanced Surface Ablation / Laser Assisted Sub-Epithelial Keratectomy (LASEK)/ Photorefractive keratectomy
(PRK)
ⅳ. Small Incision Lenticule Extraction (SMILE)
ⅴ. Radial keratotomy (RK) / Astigmatic keratotomy (AK)
ⅵ. Intracorneal rings
ⅶ. Phakic Intra-ocular Lens
c. Evaluation and identification of postoperative complications
ⅰ. Interpretation of postoperative corneal topography
ⅱ. Interpretation of patients’ symptomatology
ⅲ. Management of complications
d. Understand the effect of corneal refractive surgery on intraocular lens calculation
2. Glaucoma
Topics to be covered in Basic Ophthalmology Training
a. Perform slit lamp biomicroscopy, including assessment of anterior chamber depth
b. Perform IOP measurement with Goldmann applanation tonometry, handheld transducer-based tonometer, and
rebound tonometer
c. Perform bleb assessment, including Seidel test for aqueous leak
d. Perform optic disc assessment (e.g. cup-disc ratio, cup morphology)
e. Perform gonioscopy, including indentation gonioscopy
f. Interpretation of visual field tests
g. Interpretation of retinal nerve fiber layer analysis (e.g. using OCT)
h. Interpretation of anterior segment OCT
i. Interpretation of visual field tests
j. Interpretation of retinal nerve fiber layer analysis (e.g. using OCT)
k. Interpretation of anterior segment OCT
Topics to be covered in Higher Ophthalmology Training
a. Perform laser trabeculoplasty
b. Perform transscleral cyclophotocoagulation
c. Assist or perform glaucoma filtration surgery, and/or implantation of glaucoma drainage devices (GDD)
b. Early postoperative management after filtration surgery or GDD implantation:
ⅰ. Hypotony, including assessment for associated complication (e.g. maculopathy)
ⅱ. Reformation of the anterior chamber
ⅲ. Interventions for bleb leak
ⅳ. Laser suture lysis
e. Use of antifibrotic agents after filtration surgery, including their subconjunctival injection
f. Assist or perform bleb needling
g. Knowledge of minimally invasive glaucoma surgery (MIGS)
3. Neuro-ophthalmology
Topics to be covered in Basic Ophthalmology Training
a. Assessment of
a. eye movement, including cover/uncover/alternating/prism cover tests, Hirshberg and Krimsky tests
b. pupils, including pharmacologic testing
c. eyelids malposition
d. proptosis including exophthalmometry
b. Neurological examination in relation to ophthalmology, including other cranial nerves and cerebellar signs
c. Interpretation of orthoptic reports, e.g. Hess chart, tests of binocularity and fusion, use of prisms
d. Manual and automatic perimetry: indications, perform and interprets results
e. Indications for and interpretation of ocular and neuroimaging in relation to neuro-ophthalmology
f. Perform icepack test for myasthenia gravis. Know the indications and potential complications of Tensilon and
Neostigmine tests
g. Recognize and provide initial management for emergent neuro-ophthalmic conditions
h. Know the indications, and be familiar with the complications and monitoring, of the use of corticosteroid for the
treatment of inflammatory neuro-ophthalmic diseases.
Topics to be covered in Higher Ophthalmology Training
a. Recognize and diagnose common afferent and efferent neuro-ophthalmic diseases
b. Understand and perform clinical tests for functional visual loss
c. Perform forced duction and force generation tests
d. Perform botulinum injections for blepharospasm, hemifacial spasm and upper lid retraction
e. Observe temporal artery biopsy, if available
f. Know the indications for, observe and interpret electro-diagnostics tests (e.g. visual evoked potential,
electroretinogram) for evaluation of optic nerve disorder and visual loss of unknown cause
g. Know the indications and be familiar with the complications and monitoring, of the use of immunosuppressants
(including biologic agents) for the treatment of inflammatory neuro-ophthalmic diseases.
4. Oculoplastic and Orbit
Topics to be covered in Basic Ophthalmology Training
a. Topics to be covered in Basic Ophthalmology Training
b. Assess eyelid, orbital and lacrimal system disorders
a. eyelid malposition, ptosis
b. proptosis, thyroid eye disease
c. epiphora
c. Interpret orbital and relevant sinus anatomy on imaging studies
d. Perform minor eyelid/ lacrimal system procedures:
ⅰ. lid laceration repair
ⅱ. small eyelid lesion incisional or excisional biopsy
ⅲ. chalazion curettage
ⅳ. temporary tarsorrhaphy
ⅴ. trichiasis correction (electrolysis, cryotherapy)
ⅵ. syringing and probing
ⅶ. incision and drainage of lacrimal sac
Topics to be covered in Higher Ophthalmology Training
a. Comprehensive knowledge of eyelid, orbital and lacrimal system anatomy, related diseases, and pathology
b. Understand the fundamentals of common periocular aesthetic procedures (botulinum toxin, fillers,
radiofrequency, focused ultrasound, laser etc.) and their possible complications
c. Perform
a. botulinum toxin injection for blepharospasm
b. surgical correction of entropion/ ectropion
c. lateral canthotomy/ cantholysis
d. Perform with supervision or assist
ⅰ. evisceration/ enucleation
ⅱ. upper eyelid blepharoplasty
ⅲ. ptosis correction
e. Perform with supervision or assist
ⅰ. eyelid reconstruction
ⅱ. orbital surgery (tumor biopsy/ removal, fracture repair, decompression)
ⅲ. lacrimal surgery
• dacryocystorhinostomy (external or endoscopic)
• silicone tube insertion and removal
• Jones tube insertion
5. Paediatric Ophthalmology and Strabismus
Topics to be covered in Basic Ophthalmology Training
a. Perform assessment of vision in neonates, infants, and children
b. Perform ocular motility examination
c. Perform cycloplegic refraction in children
d. Binocular vision assessment – sensory and motor
e. Interpretation of orthoptic assessment report, including Hess chart. Prescribe prismatic glasses
f. Assist in performing extraocular muscle surgery and paediatric eyelid surgery
g. Understand the options of myopia treatment in paediatric patients
Topics to be covered in Higher Ophthalmology Training
a. Perform assessment of vision in more difficult patients (uncooperative patients, mentally impaired and non-
verbal)
b. Knowledge in using and monitoring of chloral hydrate sedation for examination
c. Perform forced duction test
d. Assist or perform strabismus surgery (both paediatric and adult strabismus) –muscle strengthening
and weakening procedure, e.g., recession and resection, as well as adjustable surgery, and botulinum toxin injection
to extraocular muscles
e. Assist or perform paediatric eyelid surgery, such as epiblepharon correction or ptosis correction
f. Assist or perform syringing +/- probing of nasolacrimal duct in children
g. Understand the options of myopia treatment in paediatric patients
h. Acquire skill of using indirect ophthalmoscope to assess retinopathy of prematurity and assist in retinopathy of
prematurity treatment (indirect diode laser or anti-VEGF injection)
i. Rare paediatric eye diseases (e.g. congenital anomalies and metabolic disorders)
6. Vitreoretinal Diseases
Topics to be covered in Basic Ophthalmology Training
a. Examine the fundus of the eye using appropriate techniques and accurately interpret the findings.
b. Perform and interpret fundus photography, OCT and B-scan ultrasonography.
c. Interpret fluorescein and indocyanine green angiography
d. Understand the indications, risks, and limitations of laser treatment. Apply appropriate laser for the management
of retinal disorders
e. Perform pan-retinal photocoagulation
f. Perform laser retinopexy for retinal breaks
g. Perform anterior chamber and vitreous tapping for diagnostic purposes
h. Perform intravitreal injection of medications
i. Know the indications, and be familiar with the complications and monitoring, of the use of corticosteroid
(different routes of delivery) for the treatment of ocular inflammatory diseases.
Topics to be covered in Higher Ophthalmology Training
a. Perform focal and grid macular laser treatment
b. Perform posterior subtenon and/or orbital floor injection of corticosteroid
c. Assist cryopexy of retinal breaks
d. Assist in scleral buckling procedures and pars plana vitrectomy procedures
e. Perform photodynamic therapy
f. Know the indications and be familiar with the complications and monitoring of the use of immunosuppressants
(including biologic agents) for the treatment of ocular inflammatory diseases.
K. Active assessment
Assessments and certifications of trainee’s competency by trainers are carried out throughout the training. They are required to be submitted to the College, include a minimum of:
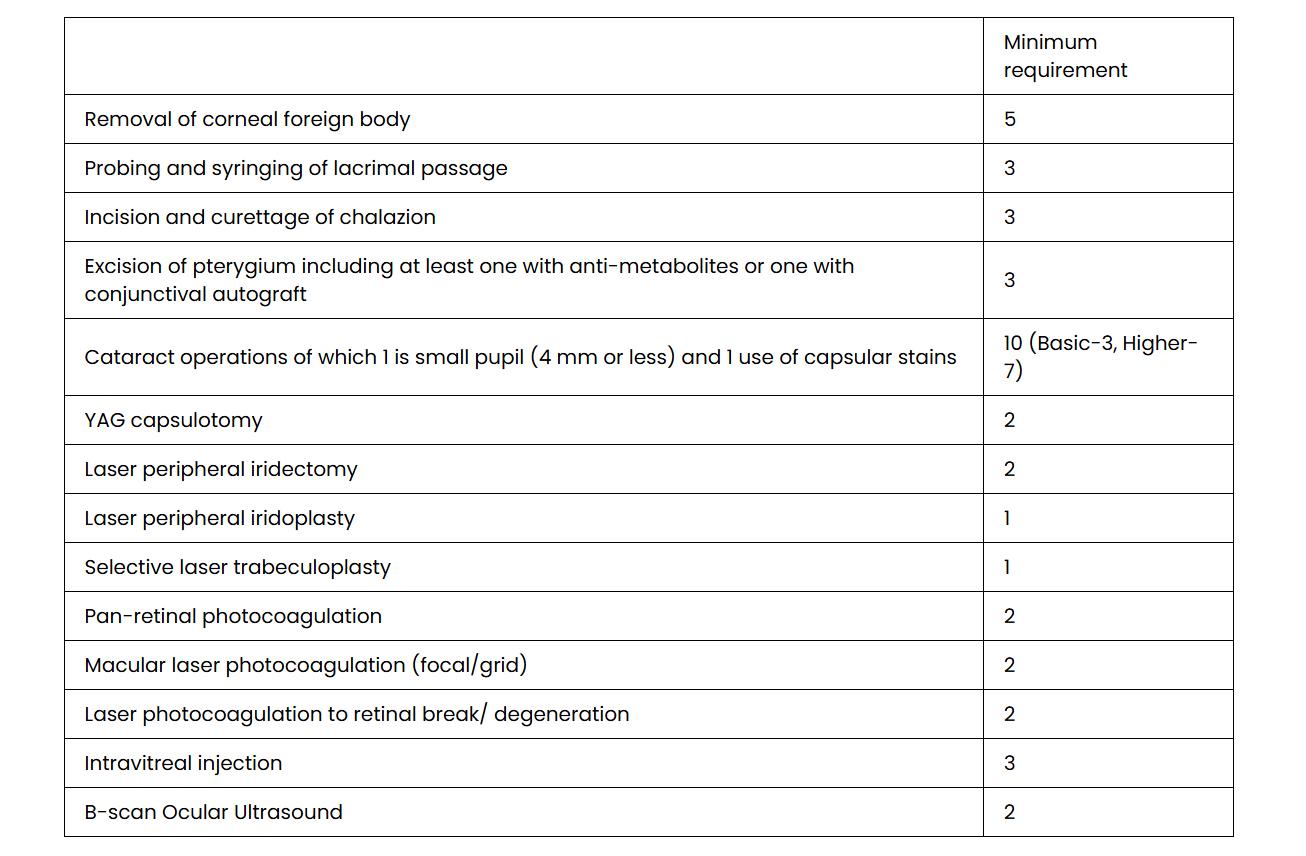
The number of each procedure required in active assessment will be revised yearly by COHK if necessary.
The trainee shall fill in the relevant forms from COHK with countersignature by a recognized trainer. The trainer must be satisfied that the trainee concerned had attained a reasonable standard in performing the said procedure(s).
L. Surgical experience assessment
At the end of higher training, the surgical experience (either as 1 st assistant or chief surgeon, unless specified otherwise), should include a minimum of:
1. 200 cataract operations (100 performed as chief surgeon)
2. 100 laser operations (performed as chief surgeon), including:
a. 15 YAG capsulotomy
b. 15 laser peripheral iridotomy
c. 3 laser peripheral iridoplasty
d. 5 laser trabeculoplasty
e. 20 pan-retinal photocoagulations
f. 15 macular laser photocoagulation (focal/grid)
g. 15 laser photocoagulation to retinal break/ degeneration
3. 10 intravitreal injections (performed as chief surgeon)
4. 15 squint operations (not including botulinum toxin injection to extraocular muscles; bilateral simultaneous surgery
count as one operation)
5. 20 glaucoma operations (up to 5 needling/bleb repair or revision/goniotomy and up to 3 transcleral
cyclophotocoagulation)
6. 15 vitreoretinal operations
7. 3 keratoplasty operations
8. 15 oculoplastic or orbital operations
9. 3 repair of ruptured eyeball operations
The minimum surgical experience will be revised by COHK periodically if necessary.
The operative results and the complications should be entered into the logbook for inspection during the exit examination.
M. Appendix
1. Provisions for part-time trainers
a. General trainer qualification: As per E.1.a.: “A trainer should have at least 2 years full-time (or equivalent) working
experience in COHK-recognized training centers after obtaining Fellowship of COHK (or the status of Specialist in
Ophthalmology from the Medical Council of Hong Kong.)” Part-time work experience can be recognised towards
general trainer qualification, provided the prospective trainer works no less than 50% in a training centre and the
duration of work experience is prolonged accordingly. E.g. a part-time ophthalmologist who works 50% in a
training centre, needs to work for 4 years post-fellowship before qualification as a trainer.
b. A COHK-recognized training centre must have a minimum of 5 full-time trainers. specialized in the field of
ophthalmology. Out of the 5 full-time trainers, ONE may be full-time equivalent (FTE).
c. Two part-time trainers who work at least 50% and for at least 6 months each may be considered as one FTE
trainer, subject to approval by COHK.
2. Core Area Trainer (CAT) Qualification
a. A general ophthalmology trainer (see E1) can qualify as a CAT through one of 3 routes:
i. Current Trainers:
A trainer, who works in a core area in a training centre, can register as a CAT with COHK by 1 st July 2022. A
trainer can only qualify as CAT in a single core area through this route.
ii. Trainer status obtained on or after 1st July 2022:
1. Fellowship Route: Completion of a formal clinical hands-on COHK-approved fellowship program of no less
than 1 year in the same core area. Overseas training to be considered by COHK on case-by-case basis. The
COHK Education committee reserves the right to examine a candidate’s training record.
2. Accreditation Route: Achieve sufficient clinical experience in the relevant core area by attending clinics and
performing surgery in the specified area (see below).
b. Clinical experience required for qualification through the accreditation route:
i. Core area clinics: attend 52 subspecialty clinics in prior 2 years
• For vitreo-retinal area- all retina clinics (surgical retina/ medical retina and uveitis) are included
ii. Core area surgery: performed as independent chief surgeon or supervisor within the past 3 years (post-
FHKAM)- minimum requirement (bilateral surgery count as 1 procedure):
• Cornea & External Eye Diseases:
- Corneal grafts (any types): 20
- Intraocular lens (IOL) exchange/ secondary IOL: 10 (at least Scleral-fixated-IOL 5)
- Amniotic membrane transplant: 5
• Glaucoma: minimum 40, including:
- Trabeculectomy/ non-penetrating drainage surgery at least 15
- Glaucoma drainage devices at least 10
- Minimally invasive glaucoma surgery/ cyclophotocoagulation not more than 10 out of 40
• Oculoplastic and Orbit
- 40 eyelid surgeries
- 12 lacrimal surgeries
- 8 orbital surgeries
• Paediatric Ophthalmology and Strabismus: minimum 40
- Squint surgeries (all types of muscle surgery, excluding botulinum toxin injection) at least 25
- Eyelid surgeries (epiblepharon/ ptosis) at least 10
- Paediatric cataract surgeries (<12 years): at least 2
- Miscellaneous: syringing and probing, retinopathy of prematurity laser/ injection, examination under
anaesthesia (no minimum of each)
• Vitreo-Retinal Diseases
- 50 retinal detachment surgeries (vitrectomy and/or buckle)
- 30 macular surgeries (epiretinal membrane or macular hole)
c. CAT qualification for ophthalmologists not working in COHK training centres
i. Ophthalmologists who have qualified as a trainer and work in a core area before 1 st July 2022- can apply for
CAT eligibility at the initial implementation of this scheme in 2022. The application process will involve a
declaration countersigned by the candidate’s previous training centre’s COS (or equivalent) and subjected to
vetting by COHK. This eligibility can be retained indefinitely in the future. For those who apply later than 1 st July
2022- they can only gain CAT eligibility by fellowship or accreditation routes. CAT eligibility is for training only. It
does not equate subspecialist status and is not quotable.
ii. For trainers who gained CAT status after 1 st July 2022 in training centres then leave the training centre, they
can retain CAT eligibility.
iii. If a trainer has not attained CAT status before 1 st July 2022 and leaves the training centre before fulfilling the
accreditation requirements, he/she can gain CAT eligibility by fellowship or accreditation only (taking into
account the total number of surgeries and clinics in the training centre and in the private sector within the set
period).
iv. The accreditation criteria (number of clinics and surgeries) are the same for trainers in training centres and in
the private sector.
v. Other cases to be considered by COHK on a case-by-case basis.
d. Once an ophthalmology specialist becomes a CAT, no revalidation is necessary unless he/ she decides to
change major core areas/ or wishes to act as CAT in 2 core areas.
e. Dual core areas: If a CAT would like to be a trainer in 2 core areas, the CAT qualification must be gained by
accreditation or fellowship routes in both areas and subjected to revalidation every 2 years. (The revalidation
requirement is the same as the accreditation criteria). Such trainers can supervise one HOT in either one core
area at any given time.
f. The list of trainers who have CAT status or eligibility will be kept by COHK (not open to public).